When the Jaw Blocks Healing: FDOJ and Silent Toxins in Lyme Disease
Attached to every dead tooth is an exceedingly sick individual. This phrase might sound deeply dramatic at first — but in biological medicine, it consistently reveals itself as harsh, measurable anatomical reality. Throughout my decades of clinical practice, I have witnessed hundreds of severely debilitated Lyme disease patients where meticulously applied antibiotic regimens failed completely. The underlying reason? Massive, silent toxic blockages situated right above the neck line. Without a profound understanding of FDOJ and devitalized teeth, the healing of chronic neuro-inflammation is usually an impossible battle against windmills.
The Silent Toxin Core: What is FDOJ?
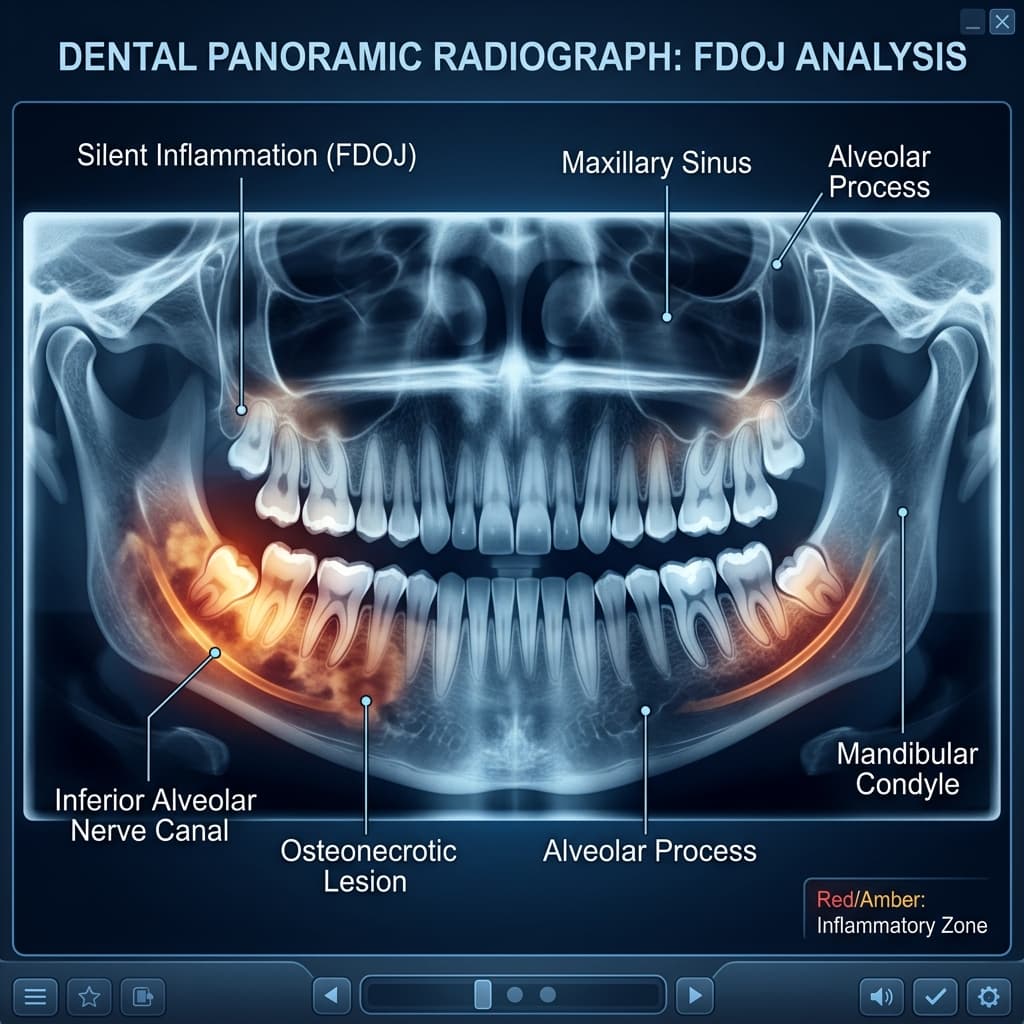
FDOJ is the strict medical acronym for — an ischemic (blood-lacking), fatty degenerative decay of the jawbone. Within these intensely toxic areolas, healthy, firm trabecular bone structure has completely melted away, having been tragically replaced by yellowish, necrotic fatty and purulent tissue.
The absolute most insidious aspect of this deep necrosis: It is almost always a perfectly silent, painless inflammation. The patient senses no local pain whatsoever, the external gum margins appear pink and incredibly healthy, and, fatally, on a classic 2D dental panoramic X-ray (OPG), these huge bone cavities largely remain entirely invisible. The unsuspecting patient — and often their treating dentist — remains oblivious to the toxic volcano simmering beneath the tissue.
The RANTES/CCL5 Immune Collapse
Clinical tissue biopsies and extensive analyzes forcefully confirm: Inflamed FDOJ cavities in the jaw manufacture titanic quantities of the hyper-inflammatory signaling chemokine RANTES (CCL5). The non-stop flooding of the patient's bloodstream with RANTES sends their global immune system into a catastrophic, permanent alarm state. Frontline immune cells (macrophages) are obsessively chained to the head area, causing the systemic defense against agile Borrelia spirochetes across the remainder of the body to practically collapse entirely.
Root Canals (Dead Teeth): Bacterial Bunkers in the Bloodstream
A root-canal treated tooth is a pure surgical paradox: It represents the sole actively dead biological organ tissue that the medical industry consciously leaves fixed inside the human body rather than rejecting and removing it. By permanently extracting the primary living dental nerve (pulp), the entire tooth dies. It is immediately and irrevocably cut off from the host's natural immune system.
The tremendous problem: What physically remains inside the dead tooth structure are countless thousands of dentinal tubules — microscopic, highly fibrous channels penetrating the tooth bone, which, if aligned, stretch for kilometers. Inside these dark, entirely un-policed tunnels, viciously pathogenic anaerobic bacteria begin to aggressively colonize. Because neither circulatory blood nor our body's defensive white blood cells can ever penetrate the dead tooth structure again, these resilient microbes multiply completely unobstructed.
Injecting Necrotic Toxins into the Blood
The bacteria entrenched securely inside the root canal tubules endlessly decompose protein material, excreting violently toxic metabolic waste products — predominantly fatal thioethers and highly aggressive mercaptans. Every single time the patient bites down during chewing, immense mechanic pressure actively squeezes these potent neuro-toxins forcefully down through the root tip, directly into the lymphatic system and the systemic bloodstream. Once in circulation, they effortlessly cross the rigid blood-brain barrier.
Diagnostics: Making the Silent Foci Visible
3D-CBCT (Cone Beam Computed Tomography)
The undisputed gold standard in modern holistic diagnostics. Only high-resolution 3D volumetric images can reliably visualize the dangerous trabecular breakdowns and hidden necrotic voids of FDOJ lesions. It remains an absolute requisite for every therapy-resistant Lyme patient struggling with deep neurological symptoms.
CaviTAU Ultrasound Densitometry
A highly specialized, completely radiation-free ultrasound device which meticulously measures altered, mushy bone density within the jawbone matrix. It elegantly and non-invasively pinpoints the exact locations of necrotic cavities with surgical precision.
Immunological Lab Evaluation (Toxicology)
Systemic whole-blood chemistry specifically screening for hyper-elevated RANTES/CCL5, as well as mercaptan and thioether sensitization tests. This objectively establishes the exact degree of silent systemic host toxicity.
Dental Amalgam: The Ultimate Neurotoxin
Classic black "silver fillings" made of amalgam shockingly consist of over 50% raw mercury by weight — arguably one of the most aggressively toxic neuro-poisons definitively known to humanity. For decades, it was falsely asserted that the elemental mercury remained "stably chemically bound" within the tooth filling. Strict modern spectroscopy physically proves the exact opposite: Due to abrasive toothpaste, hot beverages, nocturnal teeth grinding, and acidic milieu, measurable clouds of mercury actively off-gas and vaporize into the oral cavity every single day. These gaseous toxic vapors effortlessly bypass all lung and cellular membranes. The mercury violently inhibits hundreds of vital metabolic enzymes, paralyses active T-lymphocytes, and ironically, actively protects rampant Candida fungus and Lyme spirochetes from normal innate immune surveillance.
SMART Protocol: Crucial for Safe Removal
Dental amalgam must under absolute no circumstances ever be casually "drilled out" without maximum biological protection! Unprotected, high-speed drilling momentarily multiplies the neuro-toxic mercury exposure tenfold — frequently causing devastating, irreversible neurological crashes in already weakened patients immediately post-procedure. Seriously ill patients must exclusively demand the strict SMART (Safe Mercury Amalgam Removal Technique) protocol: 1. External medical oxygen mask supply, 2. specialized Clean-Up suction caps, 3. non-latex Rubber Dam isolation, 4. specialized carbide low-speed burs combined with massive continuous cold water suppression.
Dr. Kufahl's Conclusion
Consistent, highly diligent holistic remediation of the oral cavity is unequivocally the definitive “game-changer” in late-stage Lyme disease recovery. Profoundly hidden FDOJ necrotic cavities, decaying devitalized root canals, and chronic amalgam exposures represent titanic, unrelenting chemical blockers to the immune system. Only a highly specialized, surgically guided excision of these silent necroses combined with powerful biological adjunctive support (Medical Ozone therapy, high-dose intravenous Vitamin C, and advanced bone tissue regeneration utilizing PRF biomembranes) can adequately restore the chronically sick host's cellular freedom — finally empowering the resurgent physical body to effortlessly systematically destroy the remaining bacterial pathogens itself.
— Dr. med. dent. Wolfgang Kufahl, Holistic Biological Dentist & Environmental Medicine Pioneer
Scientific References
- Lechner, J., & von Baehr, V. (2015). Chemokine RANTES/CCL5 as an unknown link between wound healing in the jawbone and systemic disease. Clinical, Cosmetic and Investigational Dentistry. doi:10.2147/CCIDE.S79014
- Boyd, B. R. (2020). Endodontic failure and chronic systemic illness: The hidden dangers of root canals. Journal of Biological Dentistry. [Link]
- Mutter, J., et al. (2010). Amalgam studies: Disregarding basic principles of science. International Journal of Occupational Medicine and Environmental Health. doi:10.2478/v10001-010-0014-9
Important Notice: This article is strictly for neutral medical education and academic discussion. It does not replace professional medical advice, constitutes no binding recommendation for action, and must not be used for self-diagnosis or self-medication. Always consult your attending physician for health-related questions.